Iowa Periodicity Schedule
Iowa EPSDT Care for Kids Health Maintenance Recommendations
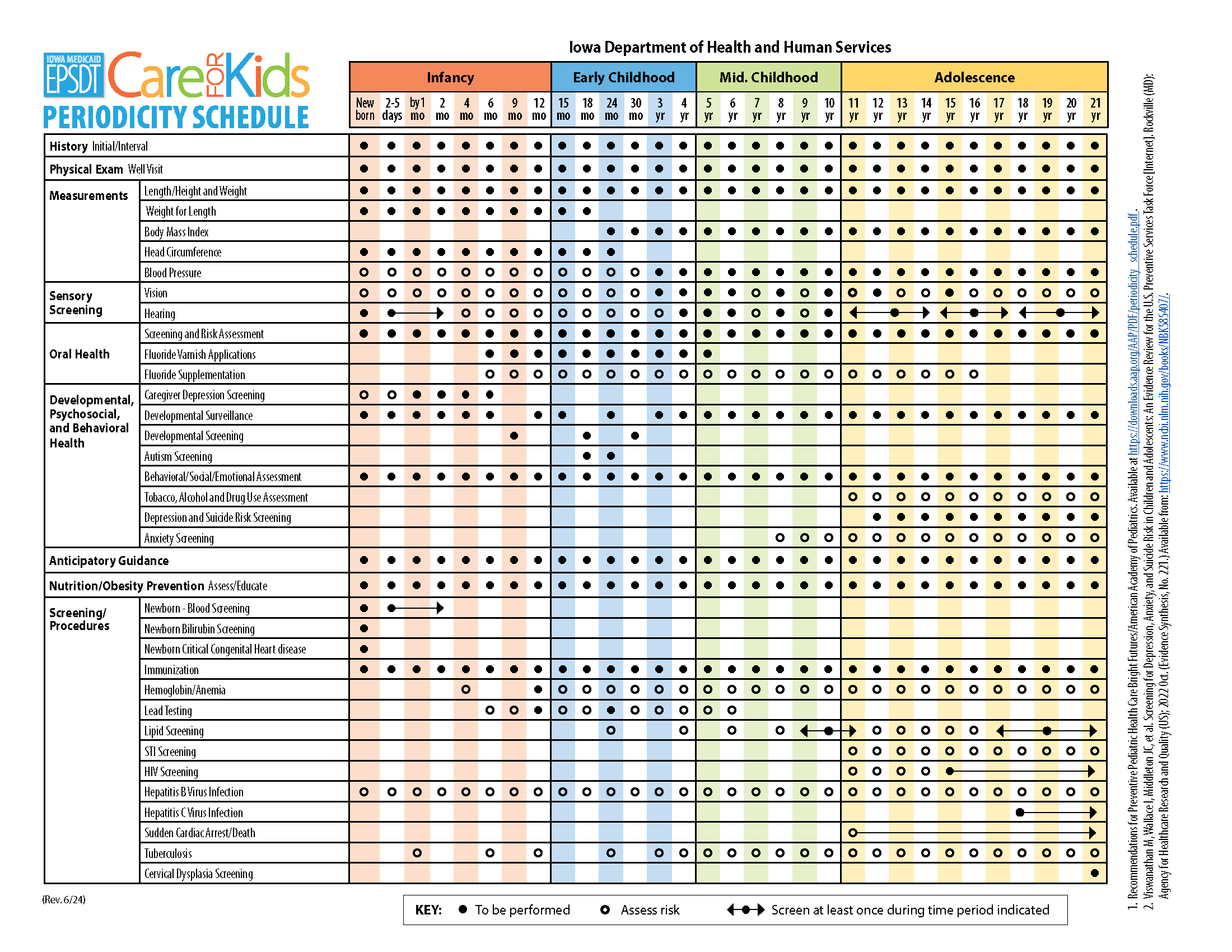
The Iowa Periodicity Schedule provides a one-page summary of the ages at which recommended health screening services are to be provided as a child grows. These guidelines are based upon Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents, 4th Edition, adopted by the American Academy of Pediatrics (AAP) and supported by Iowa's Chapter of the AAP.
Click on the image below for a printable copy of the Iowa Periodicity Schedule. Please contact us if you have questions or need help with this document.
Periodicity Schedule
Explanation 2024 - 2025
Prenatal visits: Recommended for first time parents, high risk, or if requested. The prenatal visit includes anticipatory guidance, review of family history, and discussion of the benefits of breastfeeding and plans for feeding. These visits are not reimbursable.
Birth exam: Every infant. Encourage breastfeeding and provide information.
2-5 day visit: Every infant should have an evaluation between 2-5 days of age and within 48-72 hours of discharge to include assessment for feeding and jaundice. Healthy infants discharged before 48 hours of age should be seen within 48 hours of discharge.
Thirty-month visit: A 30-month visit is strongly recommended for developmental screening. This is a good age to promote family routines, review and promote language and social development, review any concerns about behavior and/or preschool, and promote safety. Medicaid will reimburse for this visit.
Older children and adolescents: Annual screening exams are recommended by the American Academy of Pediatrics (AAP) and by Iowa Medicaid.
Physical Exam
Comprehensive histories should be taken at initial and interval well visits.
An unclothed/undressed and draped physical exam is required at each well visit, and should include an assessment of:
1) Growth:
- Use the WHO growth charts to monitor growth for infants and children ages 0 to 2 years of age in the U.S.
- Use the CDC growth charts to monitor growth for children age 2 years and older in the U.S.
2) All organ systems:
- Blood Pressure should be checked annually beginning at 3 years of age. Infants and children with risk factors should have blood pressure checked before 3 years. Access NHLBI/NIH blood pressure charts.
- Assess risk for Sudden Cardiac Arrest and sudden cardiac death to occur between 11 to 21 years old. See the AAP Summary Report: Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents
Screenings/Procedures
Newborn Screening
Note that newborn screening includes blood spot, bilirubin, hearing screening, and screening for critical congenital heart disease by pulse oximetry after 24 hours of age and before discharge. Confirm initial screen was accomplished, verify results, and follow up, as appropriate.
Hemoglobin/Anemia
Test at 12 months. Assess risk at 4 months, 15 months, and at every visit afterwards. Menstruating females are at risk for iron deficiency anemia.
Lipid Screening
Test all children once between 9 and 11 years and once between 17 and 21 years. For universal screening, non-fasting non-HDL cholesterol can be used. Assess for high risk at 24 months, and at 4, 6, 8, and 12-17 years of age. Children at big risk should be screened with a fasting lipid profile.
Immunizations
For age-appropriate immunizations, follow CDC Immunization Guidelines. Every visit should be an opportunity to update and complete a child's immunizations.
Lead Screening
The Centers for Disease Control and Prevention (CDC) updated the blood lead reference value (BLRV update, October, 2021) from 5.0 μg/dL to 3.5 μg/dL (micrograms per deciliter) to identify blood levels that are higher than most children’s levels.
The Iowa Department of Health and Human Services (Iowa HHS) has revised its Childhood Lead Poisoning Risk Questionnaire Tool and Blood Lead Testing Guidelines to help providers determine a child’s level of risk for lead poisoning. Administer blood lead level testing:
For all children: test at 12 and 24 months.
For children at higher risk: test at time high risk is determined and at 12, 18 and 24 months, then annually up to age of 6 years.
Blood lead tests: a blood lead test result equal to or greater than 15 ug/dl obtained by capillary specimen (finger stick) must be confirmed using a venous blood sample.
The CDC now considers a blood lead level of 3.5 mcg/ml elevated.
For questions, call 1-800-972-2026.
STI and HIV Screening
Adolescents should be screened for sexually transmitted infections as per recommendations in the AAP Red Book. The American Academy of Pediatrics recommends HIV screening for all 15 to 21 year olds. Sexually active adolescents should be tested annually. Iowa Code 141A.7 grants minors the legal capacity to consent to HIV-related medical care, including testing, without needing parental consent, and allows them to apply for voluntary HIV testing, treatment, and other services directly to licensed health professionals. However, they must be informed prior to testing that a positive HIV-related test result must be reported to the minor’s legal guardian.
Cervical Dysplasia Screening
Adolescents are no longer routinely screened for cervical dysplasia until 21 years of age. The AAP statement Gynecologic Examination for Adolescents in the Pediatric Office notes the indications for pelvic examinations prior to age 21 years.
Hepatitis B Screening
Assess the risk for HBV infection to occur between newborn and 21 years old. Refer to the U.S. Preventive Services Final Recommendation Statement, Hepatitis B Virus Infection in Adolescents and Adults: Screening.
Tuberculosis Testing
Annual testing is recommended for high risk groups, which include household members of persons with TB or others at risk for close contact with the disease; recent immigrants or refugees from countries where TB is common (e.g., Asia, Africa, Latin America, Pacific islands and former Soviet Union); migrant workers; residents of correctional institutions or homeless shelters; persons with certain underlying medical disorders. Children with HIV and incarcerated adolescents should be tested yearly. Visit the Iowa HHS website for more information on Tuberculosis (TB) Control.
Developmental and Behavioral Health
Developmental surveillance
Developmental surveillance is required for every health maintenance visit and is not separately reimbursable. Developmental surveillance consists of reviewing family and child strengths and risk factors, eliciting caregiver concerns, reviewing developmental milestones, observation of the child, monitoring and anticipatory guidance.
Developmental Screening
Any child who is identified as having a developmental concern should undergo developmental screening using a standardized screening tool. If potential developmental concern is noted, child should be referred immediately for more in-depth diagnostic evaluation.
Perform Developmental Screening at 9, 18 months, and 24-30 months. The Ages and Stages Questionnaires, Third Edition (ASQ-3) is the suggested tool. Medicaid will reimburse for use of a standardized screening tool (billing code 96110).
Perform Autism Screening at 18 and 24 months. A number of autism screening tools have been developed and are commonly used. AAP provides a list of links to tools for developmental surveillance and screening, including the Modified Checklist for Autism in Toddlers-R/F (M-CHAT-R/F). Medicaid will reimburse for use of a standardized screening tool (billing code 96110). Any child suspected of autism spectrum disorder should be referred immediately for services, diagnostic evaluation, and receive an audiological evaluation.
Behavioral Screening
Assess children and adolescents for depression, anxiety and suicide risk between the ages of 8 and 21. AAP/Bright Futures recommends screening of children and adolescents for depression beginning at 12 years of age.
The Patient Health Questionnaire-2 (PHQ-2) is a brief and practical tool to use. If screening is positive on the PHQ-2, the PHQ-9 should be administered. Medicaid will reimburse for the PHQ-9 or other standardized tool. The PHQ-2 is not a separately reimbursable service.
Family Risk Factors
Assess family risk factors using the Bright Futures Pediatric Intake Form.
For caregiver depression screening, Medicaid will reimburse for using the Edinburgh Postnatal Depression Scale or the Patient Health Questionnaire 9 (PHQ-9).
- Edinburgh Perinatal Depression Scale
- Patient Health Questionnaire (PHQ9 & PHQ2) Overview
- PHQ Screeners
The CMS Center for Medicaid and CHIP provides information about prevention and early identification of mental health and substance use conditions: Mental Health and Substance Use Disorder Services
Tobacco, Alcohol and Drug Use Screening: AAP/Bright Futures recommends screening for alcohol, tobacco, and substance use annually, beginning at 11 years of age by asking directly about usage or experimentation. See Substance Use Screening, Brief Intervention, and Referral to Treatment for Pediatricians. The CRAFFT screening tool is helpful for identifying problem use and is a suggested tool. Medicaid will reimburse for the use of the CRAFFT or other standardized tool.
Additional Resources
More information and resources are available on the Developmental Care and Mental Health Care pages of this website.
Sensory Screening
Vision Screening
Assess risk at every visit. Vision screening should start at 4 years of age and in cooperative 3-year-olds. Consider instrument screening at 12 and 24 months, and at 3, 4, and 5 years of age.
Iowa law requires that the parent or guardian of a child enrolled in kindergarten or third grade ensure that evidence of a child vision screening be submitted to the school in which the child is enrolled. This may be submitted in electronic form or hard copy, or electronically through Iowa Immunization Registry Information System (IRIS).
Vision screening can be performed in several settings, including healthcare provider’s office. The vision screening can be done up to one year prior to the child’s enrollment in kindergarten or third grade, or no later than 6 months after enrollment.
More information is available from Prevent Blindness Iowa - Children's Vision Screening.
Hearing Screening
Iowa law requires universal hearing screening of all newborns and infants in Iowa. Confirm initial screen was completed, verify results and follow up as appropriate. See Hearing Assessment in Infants and Children: Recommendations Beyond Neonatal Screening and refer to Iowa's Early Hearing Detection and Intervention Program (EHDI) to learn more about EHDI program goals, and link to EHDI laws and administrative rules.
Find information aimed EHDI resources for providers. Find EHDI - educational materials and guidance for best practices for providers and families.
Iowa EPSDT recommends in-office screening using audiometry, beginning at 4 years. Screen at least once between the ages of 11 and 14 years, once between 15 and 17 years, and once between 18 and 21 years, using audiometry to include frequencies between 6000-8000 HZ.
Oral Health
An examination of the oral cavity and dentition, and teaching about oral/dental health care should occur at every visit. Refer to dental home by 12 months or within 6 months of eruption of first tooth. Ask about dental home at every visit.
I-Smile Dental Home Initiative
Iowa law requires that children under the age of 12 years who receive Medicaid must have a dental home. The I-Smile Dental Home Initiative was created to assist with locating, training and matching children, particularly young children, with dental providers in Iowa. They use dental hygienist care coordinators to assist physicians and families find dental homes.
Medicaid Dental Periodicity Schedule for Children
Iowa’s Periodicity Schedule of Dental Services for Medicaid-enrolled children identifies the types of services recommended based upon the age of a child and risk for dental disease. The recommendations were developed using information from the American Academy of Pediatric Dentistry and also Iowa’s definition of a dental home.
Download a pdf of the Iowa Medicaid Dental Periodicity Schedule for Children.
New Oral Health page
The Care for Kids website has a new page for Oral Health Care information. Find additional information on:
- Medicaid Dental Home
- I-Smile Initiative
- Caries Prevention
- Fluoride Varnish
- Water Fluoridation
Anticipatory Guidance
Resources and Materials to Share with Families
EPSDT encourages providers to offer practical and contemporary health information to parents before significant physical, emotional and psychological milestones. This guidance will help parents anticipate impending changes and take action to maximize their child’s developmental potential and identify their child’s special needs.
- Bright Futures is a joint initiative of HRSA's Maternal and Child Health Bureau and the Academy of Pediatrics. The initiative offers comprehensive health supervision guidelines and tools, including recommendations on immunizations, routine health screenings and anticipatory guidance. They also provide free resources for families, and children and teens.
- Zero to Three: Materials for parents and providers, including child development handouts for parents that discuss development from the child’s perspective.
- Ages and Stages: A series of downloadable brochures on child development based on age from Iowa State University.
- Essentials for Parenting: This CDC website provides information and materials to help parents develop strong, stable and nurturing relationships with their children. Find resources specific to toddlers & preschoolers, or teens.
Transitioning to Adult Healthcare
The Academy of Pediatrics recommends that transitioning to adult healthcare begin at 12 years of age. Find more about the transition from adolescent to adult health care from the AAP's Transition Resources.
The Got Transition website is an excellent resource for professionals, teens and families. It covers all aspects of transition planning.
Nutrition/Obesity
At every visit, assess nutrition and obesity. Refer to the AAP Institute for Healthy Childhood Weight. Provide anticipatory guidance and intervention, as needed.
Website Accessibility
Iowa EPSDT is committed to making our information and materials accessible to everyone.
To increase the font size on site pages, hold down CTRL and press + on a PC. Hold down Command and press + on a Mac.